
Employee Benefit Election Form Template, Free 11 Employee Election Forms In Pdf Ms Word
Employee benefit election form template Indeed recently has been hunted by users around us, perhaps one of you. People now are accustomed to using the internet in gadgets to view video and image information for inspiration, and according to the title of this article I will talk about about Employee Benefit Election Form Template.
- University Human Resources Benefits Open Enrollment
- Death Survivor Benefits The Western Conference Of Teamsters Pension Trust
- Company Transfer Letter Template 6 Free Word Pdf Format Download Free Premium Templates
- Termination Checklist Template 15 Free For Word Doc Pdf
- Cobra Notices And Forms
- Https Www Aicpa Org Content Dam Aicpa Interestareas Employeebenefitplanauditquality Resources Planadvisories Downloadabledocuments Ebpaqc Plan Advisory Retaining And Protecting Plan Records Pdf
Find, Read, And Discover Employee Benefit Election Form Template, Such Us:
- Http Www Explainmybenefits Com Wp Content Uploads 2017 09 2018 Benefit Election Form Pdf
- 2
- 80 Free Bootstrap Templates You Can T Miss In 2020
- Death Survivor Benefits The Western Conference Of Teamsters Pension Trust
- Change In Status Termination Election Form Section 125 Cafeteria Plan Download Printable Pdf Templateroller
If you re searching for Election 2020 Youth Townhall you've reached the right place. We have 100 graphics about election 2020 youth townhall including images, photos, photographs, wallpapers, and more. In these webpage, we also provide variety of images out there. Such as png, jpg, animated gifs, pic art, symbol, blackandwhite, translucent, etc.
Paid Family And Medical Leave Exemption Requests Registration Contributions And Payments Mass Gov Election 2020 Youth Townhall
Https Www Ibm Com Us En Employment Benefits Assets 2019 Benefits And Hr Programs Pdf Election 2020 Youth Townhall
Fillable Online Bcfs Employee Benefit Election Change Form Bcfs Org Fax Email Print Pdffiller Election 2020 Youth Townhall

Fillable Online City Of Auburn Employee Benefit Election Form Long Term Care Fax Email Print Pdffiller Election 2020 Youth Townhall

Working With Flexible Benefits Election 2020 Youth Townhall
Employee Benefit Statement Service About Us Mybenefitstatements Election 2020 Youth Townhall
Or elect not to enroll in the fehb program employees onlyor.

Election 2020 youth townhall. Plan description name for employer use only. You must make an election for each benefit even if declining coverage. Benefits effective date will be the 1st of the month following your date of hire.
All rates are effective january 1 2017. You have 30 days from the date you were hired into a benefited position to complete and return this form. Do not delay submitting this form benefits enrollmentchange form if you are waiting to receive required supporting documentation.
Notice of election forms are essential in informing persons an institution or any organization of your preference regarding their service andor the benefit coverage they provide. Health benefits election form form approved. Employee benefit election change form 1.
If an employee wants to change his previously elected benefit and personal information disclosed in his insurance policy coverage then he must fill out an employee election change form. Switch designated eligible family member. Reason for application 3.
Change of statuscoverage 5. Section 125 employee benefit election form employer. Employee signature date for hrbenefits service center use only properly completed forms along with any required documentation should be submitted to the mpc benefits service center email.
Pre tax per carrier coverage monthly premium pay period blue shield ppo high envisionrx prescription plan. December 31 2017 i have elected participation in the following benefits. Plan description name for employer use only.
Employee benefit election change form for aca compliant groups with 2 to 50 employees 1. Here are a few tips you can follow while filling out or writing these forms. The form will contain the employees name mailing address contact numbers reasons for the change and benefits description.
All rates are bi weekly. Election form is the basis upon which coverage may be issued under the plan. Social security plan year beginning.
Employee election change form. Uses for standard form sf 2809 use this form to. Room d 03 105 539 south main street findlay oh 45840 employee benefit plans.
Submit your completed signed form within 30 calendar days of hire date eligibility date or qualified life event effective date. Notice of election form guidelines. Election form is the basis upon which coverage may be issued under the plan.
January 1 2017 ending. Reason for application 3. Unitedhealthcare choose one option below.
Change of statuscoverage 2. Or enroll or reenroll in the fehb program. Employee only 3258 decline medical coverage if selected please complete employee medical declination acknowledgement on page 5.
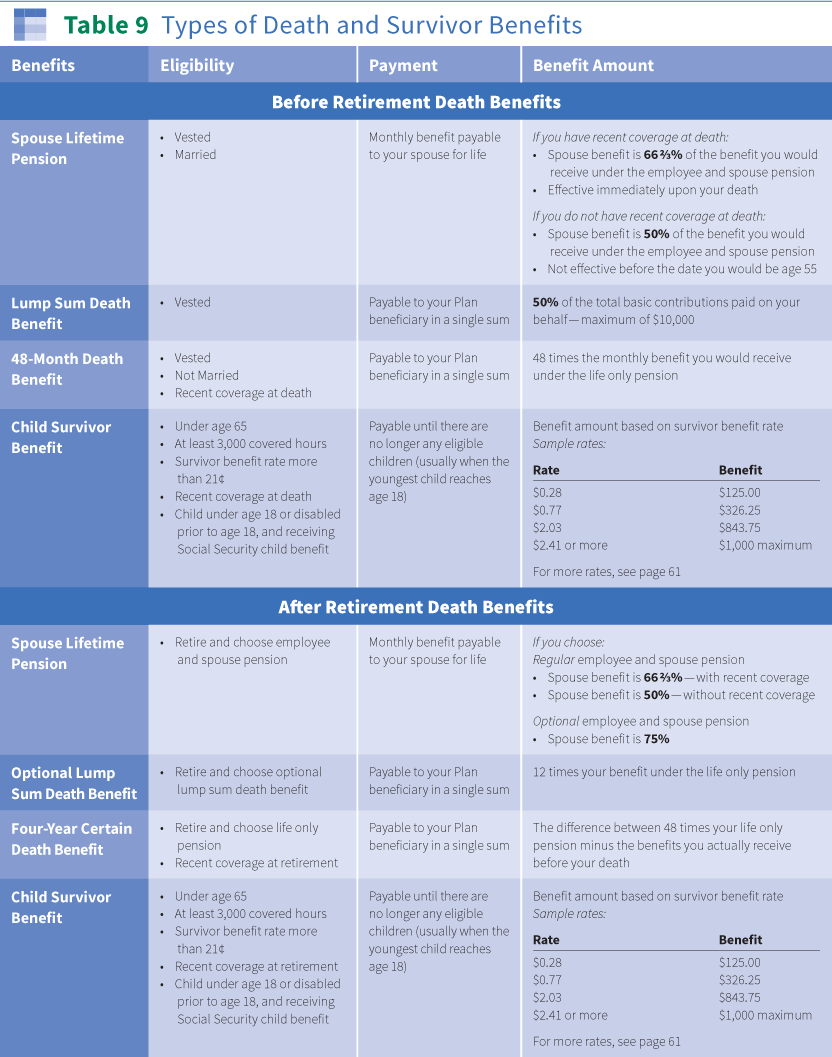
Death Survivor Benefits The Western Conference Of Teamsters Pension Trust Election 2020 Youth Townhall

Pin Di Certificate Templates Election 2020 Youth Townhall

Employee Of The Month Voting Form Template Jotform Election 2020 Youth Townhall
Election Form Template Fill Out And Sign Printable Pdf Template Signnow Election 2020 Youth Townhall
More From Election 2020 Youth Townhall
- Presidential Election Us Dates
- Presidential Election Game 2020
- Velenoso Mazza Di Tamburo
- Election Of 1876 Electoral Votes
- Kentucky Election Candidate Information
Incoming Search Terms:
- Open Enrollment Guide Resources Kentucky Election Candidate Information,
- Types Of Employee Benefits And Perks Kentucky Election Candidate Information,
- Brilliant Health Insurance Election Form Models Form Ideas Kentucky Election Candidate Information,
- Cobra Notices And Forms Kentucky Election Candidate Information,
- Free 11 Employee Election Forms In Pdf Ms Word Kentucky Election Candidate Information,
- 2 Kentucky Election Candidate Information,